Women’s Heart Disease – Why it’s an Issue
Despite heart disease being a leading cause of death in women, most women are unaware of their own risk. Women tend to delay seeking medical attention for heart attack symptoms and are more likely to die in the weeks following their heart attack than men.
Our understanding of heart disease has been based on research undertaken mainly on men. But women’s hearts and men’s hearts are different. Women have different risk factors to men, and often experience different symptoms. It is crucial that we educate women about the importance of understanding their cardiovascular risk factors, so that their risk can be minimised. Knowledge of the “atypical” heart attack symptoms that women may experience can empower women to seek help quickly should they need to.
Cardiovascular Risk Factors in Women
While high blood pressure, high cholesterol, diabetes and being overweight are known risk factors for both genders, smoking carries a higher risk in women. There are also hormonal factors that impact a woman’s risk, with early onset of menstruation (before age 10) increasing the risk of heart disease. Similarly, premature menopause (before age 50) also conveys a higher cardiovascular risk. Furthermore, women who experience pregnancy complications (such as pre-eclampsia, gestational diabetes, gestational hypertension or deliver a small for gestational age infant) are more likely to develop cardiovascular disease at a younger age.
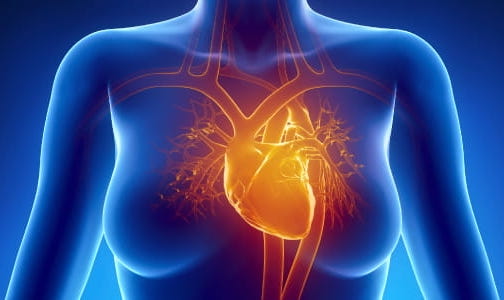
Signs & Symptoms of Heart Disease in Women
Women’s hearts are smaller, pump faster and have different sized vessels. They also have different patterns of disease to male hearts and experience different symptoms during a heart attack. While men classically experience heavy central chest pain that may radiate to the jaw or left arm, women are more likely to experience other more general symptoms such as overwhelming fatigue, breathlessness, sweating, nausea, dizziness, arm pain/heaviness, chest tightness or pressure, or heartburn-like symptoms.
Different Types of Heart Disease
Traditionally much of the cardiovascular research was conducted on men, so our understanding of what a “heart attack” looks like was based on a male type heart attack. It transpires that women often have different causes for their heart attacks, making treatment more challenging. A heart attack in simple terms is caused by an interruption of blood supply to the heart muscle so that the muscle doesn’t function properly and/or malfunctions to cause an abnormal and dangerous rhythm.
This is often caused by cholesterol build up in the arteries that leads to a narrowing (“plaque” or atherosclerosis), with sudden blockages occurring when one of the cholesterol deposits bursts. When cardiologists perform coronary angiography (a dye study of the heart vessels) blocked arteries can be identified and opened up with a stent. Women are more than twice as likely to have heart attacks without detectable blockages in their arteries at angiography. This is termed a Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA). There are many different causes of MINOCA, some of which require very different types of therapy than those implemented in classical atherosclerotic coronary artery disease.
Causes of MINOCA
1) Spontaneous Coronary Artery Dissection (SCAD)
Spontaneous Coronary Artery Dissection (a tear or bleed within the wall of an artery) causes the majority of heart attacks in women under the age of 40. SCAD is unrelated to the usual cardiovascular risk factors, but instead related to hormonal factors and, potentially, underlying abnormalities in the heart arteries. Although not always possible, SCAD is ideally managed without stents or coronary artery bypass surgery. Medications, such as beta blockers, and cardiac rehabilitation with psychosocial support are crucial management tools.
2) Coronary Artery Vasospasm
Coronary artery vasospasm is an under recognised cause of angina and heart attacks. Rather than a build of cholesterol plaque, in this condition the heart artery walls spasm or constrict inappropriately resulting in a restriction of blood supply to the heart muscle, causing angina or even a heart attack. This can be triggered by environmental factors such as cigarette smoke, stimulants, cold weather and stress, but in other cases can occur without apparent cause. Vasospasm is best managed with medications that relax the vessel walls (such as calcium channel blockers and nitrates).
3) Microvascular Dysfunction
95% of the vessels in the heart are in the extremely small vessels that can’t be visualised at the time of a conventional coronary angiogram. Women more frequently have disease of these smaller vessels or “microvasculature” and experience signs and symptoms of a heart attack or angina but at angiography no blockages are identified. There is a special type of angiogram that can be done to diagnose this condition and research is underway to develop novel therapies to aid management. Managing blood pressure, cholesterol, smoking cessation, and use of medications to relax blood vessels are all aspect of patient care as is cardiac rehabilitation.
4) Plaque Erosion
Classic heart attacks involve rupture of a cholesterol-rich plaque in a heart artery which then clots to cause an occlusion. Less commonly, plaque can erode and causing a different type of clot that can break off into smaller clots and travel down the vessel causing multiple small heart attacks. In this scenario, when coronary angiograms are performed, there are no severe blockages found and it is not always apparent as to what has occurred. This phenomenon is termed “plaque erosion” and is a common cause of myocardial infarction with non-obstructed coronary arteries (aka. MINOCA). Currently, MINOCA is treated with standard post-heart attack medications such as aspirin and other blood thinners, as well as cholesterol lowering medications. Trials are underway to determine the best therapy for this type of heart attack.